Discovery & role model
Cross-clinic workflow mapping, patient and consultation data modeling, administrator / doctor / leadership role definition, and GDPR + CCPA data-ownership posture.
Case study · HealthTech · Clinic platform
How we shipped a unified clinic management platform — a native patient iOS app, a native staff Android client, and a React web control plane with role-based admin, doctor, and leadership dashboards — that consolidated four independent clinics off scattered spreadsheets and paper into one shared system, built for healthcare operators across the United States and the European Union under GDPR and CCPA expectations from day one.
Four independent private medical clinics decided to stop running their operation out of disconnected Excel spreadsheets and paper appointment books and to share one IT backbone instead. For healthcare operators in the United States and the European Union, that fragmented model breaks the moment a patient moves between facilities: appointment data drifts, physician schedules collide, and leadership has no honest view of utilization or performance across the group. The brief was to unify patients and staff in a single platform — give patients a clean way to book and manage visits, give doctors and administrators tools that replace paperwork, and give leadership a real-time picture across all four clinics in the US and EU. Off-the-shelf clinic software failed the first test: it assumes a single practice with one front desk and could not model separate administrator, doctor, and leadership roles spanning several facilities. We built the system from first principles at YuSMP Group as a unified platform — a native patient iOS app, a native staff Android client, and a React web control plane — engineered with our custom software development practice for the US and EU markets.
A snapshot of what the clinic platform delivered across web, two mobile platforms, and a role-based access model in its first production cycle.
The platform decision dominates every other architectural choice in a healthcare build. We chose a custom system over packaged clinic software because the organization's real shape — four independent facilities sharing patients, physicians, and reporting, with distinct administrator, doctor, and leadership roles — does not fit the single-practice template that off-the-shelf products assume. The configuration tax of bending a packaged platform to multi-clinic rules typically exceeds a clean custom build, and it leaves the most operationally important behavior locked behind a vendor's roadmap. A custom platform let us model the real group, integrate the exact scheduling and role rules each clinic needed, and own the patient data end-to-end — which matters for US and EU operators that have to answer to GDPR and CCPA obligations.
The trade-off most teams underweight is data sensitivity. Packaged clinic suites rarely give granular control over who sees which patient record, and that control is precisely what makes a multi-clinic rollout safe. Building the clients ourselves meant role-based access, the appointment-conflict engine, and verified-review gating were first-class concerns rather than plugins, and the entire stack — web control plane, patient app, staff app — is open and maintainable for the long run.
| Dimension | Custom platform (this build) | Off-the-shelf software | Spreadsheets / paper |
|---|---|---|---|
| Multi-clinic model | Several facilities, shared patients & physicians | Single-practice assumptions | None — lives in files |
| Role-based access | Admin / doctor / leadership, least-privilege | Coarse roles, limited scoping | Uncontrolled file access |
| Appointment-conflict logic | Per-physician, per-clinic, multi-step booking | Generic calendar slots | Manual double-booking risk |
| Verified patient reviews | Gated to actual visitors only | Often open or absent | N/A |
| Leadership analytics | Live performance & reporting across group | Per-practice, often batch | None |
| Data ownership (GDPR / CCPA) | Full ownership and residency control | Vendor-hosted, shared tenancy | Uncontrolled |
| Patient self-service | Native iOS app, history & reminders | Web portal, varies | Phone & front desk only |
Platform references: Laravel documentation, React documentation, HHS HIPAA reference.
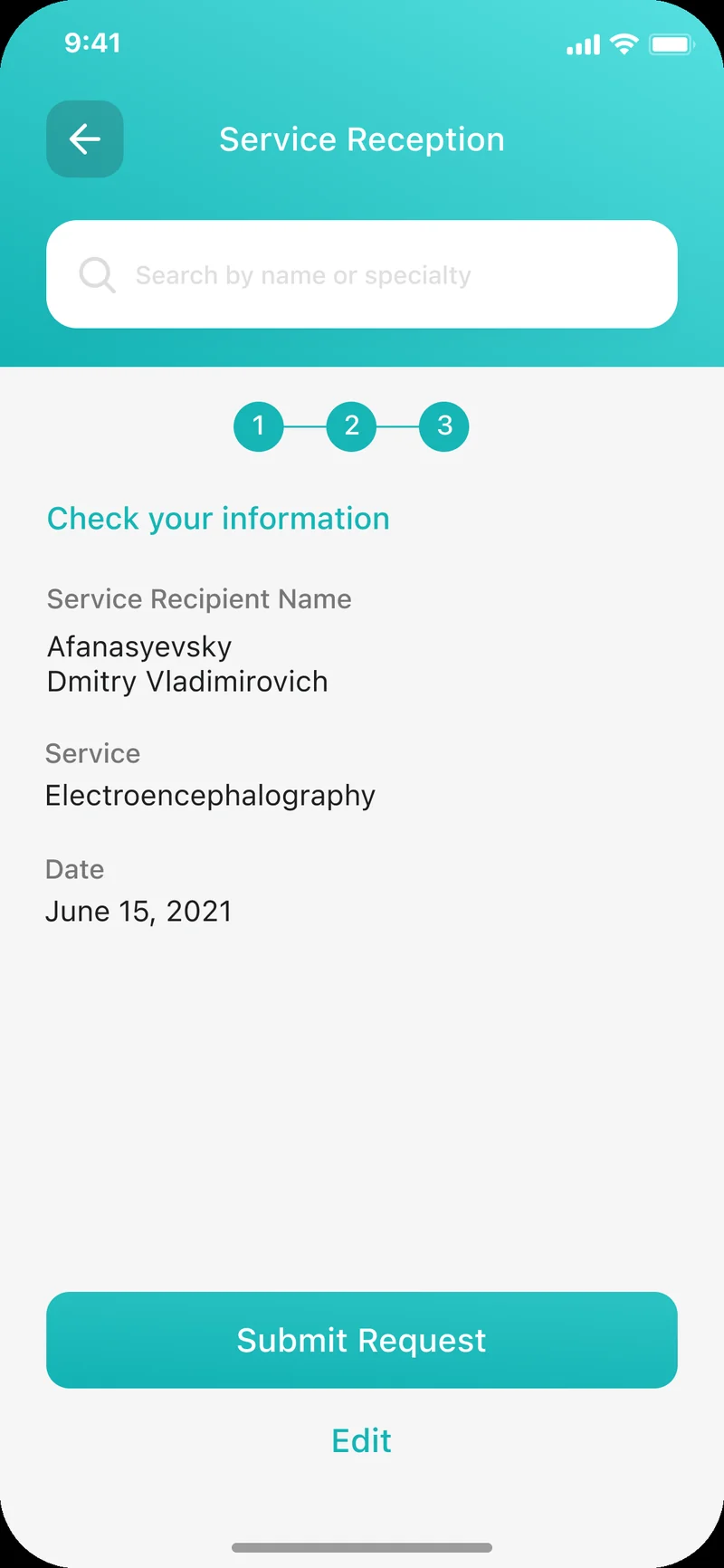
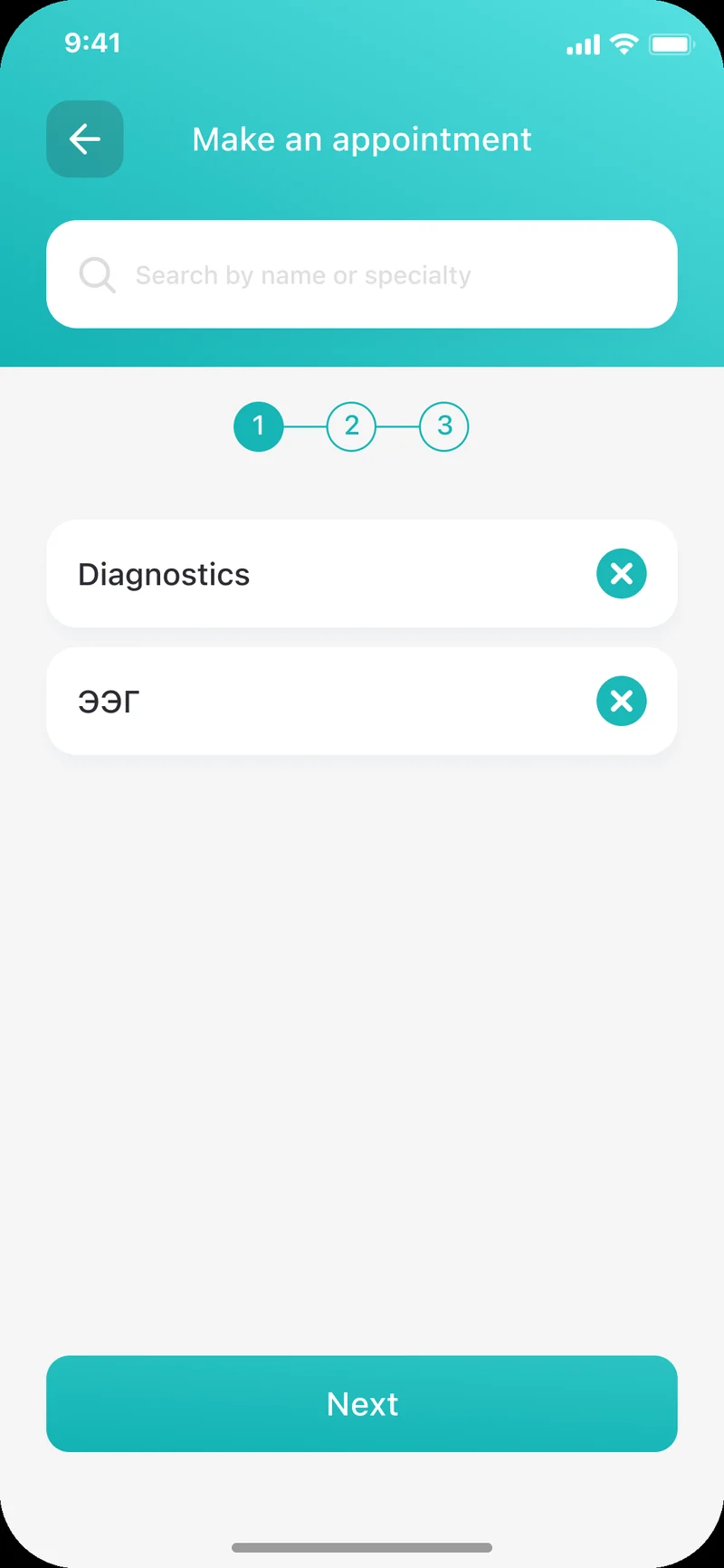
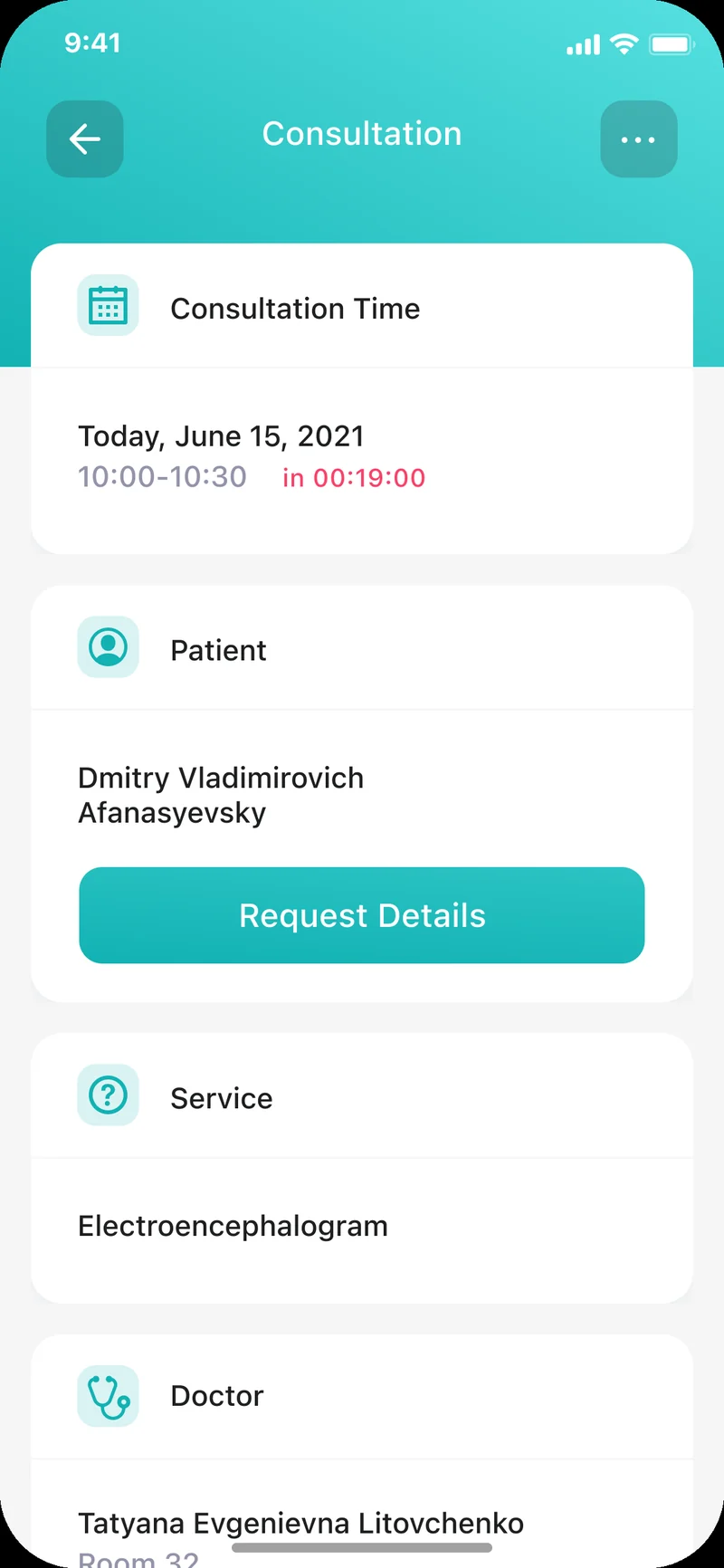
The patient-facing client is built in Swift and is the front door to the whole platform. Booking is a guided multi-step flow: a patient searches by name or specialty, picks a service such as diagnostics, chooses a physician, selects a date, and reviews a clear confirmation screen before submitting the request — so a visit is scheduled without a phone call to a front desk. The same app carries appointment history, medical recommendations, and push notifications that remind a patient of an upcoming visit, turning the clinic group's relationship with each patient into something that lives in their pocket rather than in a call log.
Trust is a deliberate design choice: reviews are gated so only people who actually attended a visit can leave one, which keeps physician ratings honest across all four clinics. The screens assume a non-technical user with large tap targets, one primary action per step, and a visible progress indicator through the booking flow. The end-to-end iOS surface is delivered as part of our mobile app development practice.
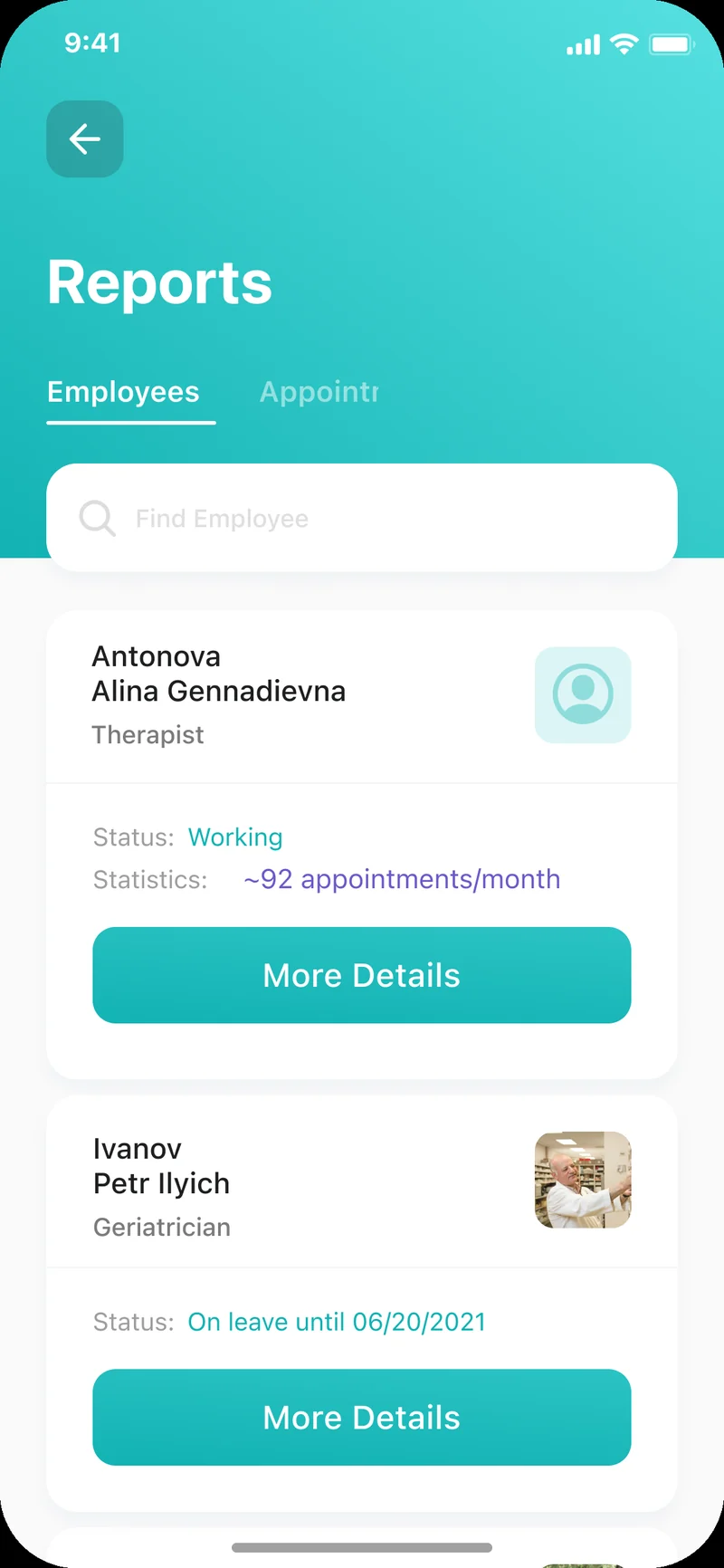
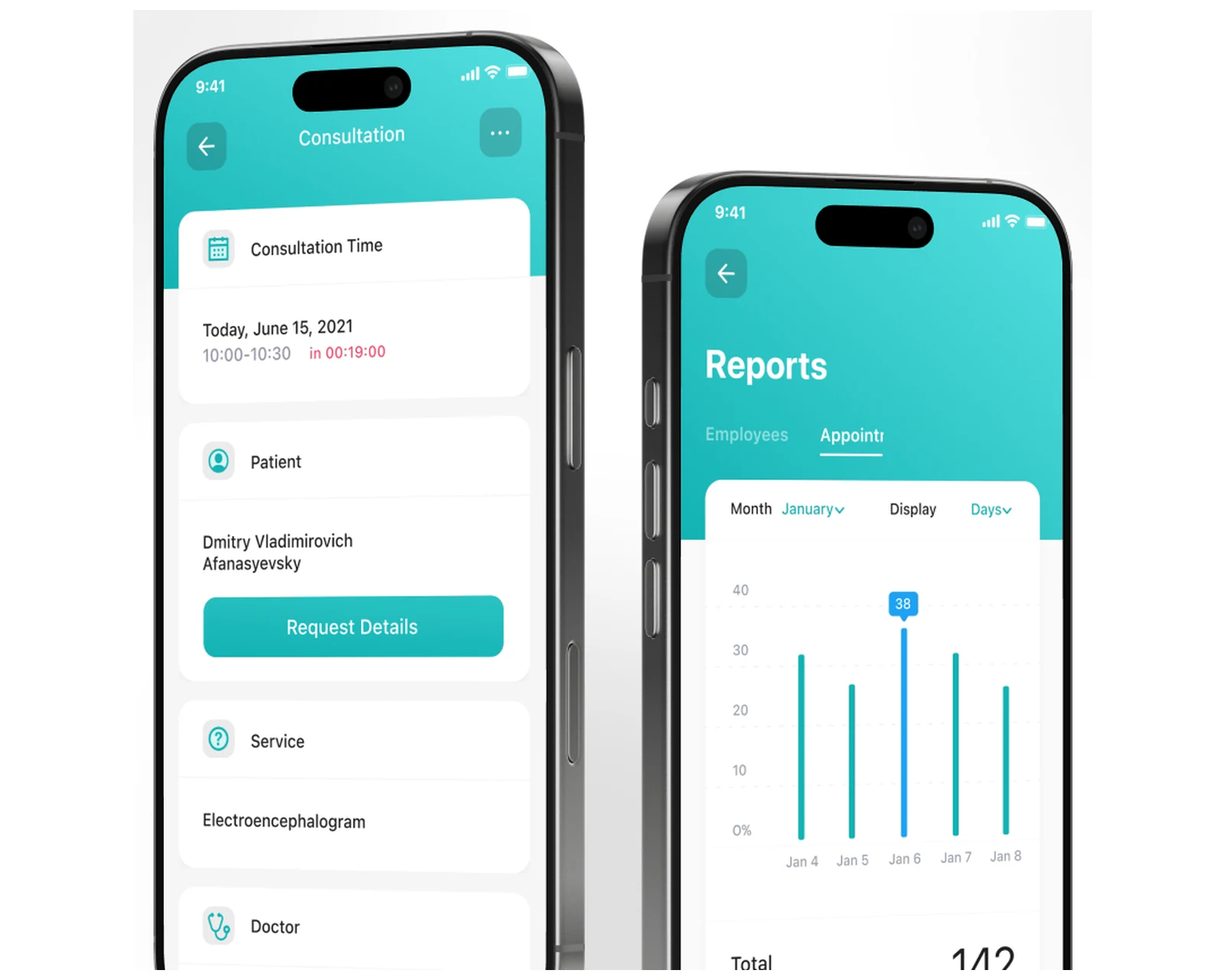
Staff needed two formats, so we built both. The native Android client gives doctors and administrators a mobile tool for work away from a desk — checking the day's schedule, opening a patient card, reviewing an employee's status and monthly appointment statistics, and confirming consultations on the move. It mirrors the booking and records model of the patient app so a single appointment is consistent on every surface. The mobile work sits inside the same iOS and Android engineering practice that delivered the patient client, so both platforms move in lockstep.
The web side is a React control plane backed by a Laravel API, and it is where office-based staff run the clinic group. Administrators manage the appointment and patient database across all four facilities, doctors open patient cards and document each visit, and the data model keeps every record in one place rather than across spreadsheets. The whole control plane is engineered on our cloud & DevOps foundation so the API, the role services, and the dashboards scale together as the clinic group grows.
Health data is the most sensitive information in the system, so role-based access is the backbone that makes a multi-clinic rollout safe. Administrators, doctors, and leadership each see only what their role requires: an administrator manages the appointment and patient database, a doctor works a personal schedule and documents consultations against a patient card, and leadership sees analytics, performance metrics, and reporting — never the raw clinical detail they do not need. Keeping these as distinct least-privilege views, rather than one shared screen with toggles, is what lets four independent facilities share one platform without leaking records between them.
Because the client owns its own deployment, data ownership and residency are design choices rather than vendor defaults. Patient data can be pinned to US or EU infrastructure for future data-residency commitments, transport and storage are encrypted, and the system aligns with GDPR obligations for users in the European Union and CCPA / CPRA obligations for users in California and the broader United States. We design for HIPAA-capable operation, but make no claim of certification that has not been independently completed — a future readiness review is a documentation exercise rather than an architectural retrofit.
Compliance posture: GDPR-aligned · ISO 27001 ready · SOC 2 Type II in progress · HIPAA-capable · CCPA-acknowledged.
A five-phase build that took four clinics from a paper-driven operation to a live web and mobile platform with role-based access.
Cross-clinic workflow mapping, patient and consultation data modeling, administrator / doctor / leadership role definition, and GDPR + CCPA data-ownership posture.
React + Laravel control plane skeleton, the multi-step appointment-conflict engine, the verified-review gate, and the role-based access contract.
Swift patient iOS app, native Android staff client, React web dashboards, patient cards, consultation documentation, and leadership analytics.
Spreadsheet and paper data import per clinic, role-based access QA, appointment-conflict testing, and data-protection review across the group.
Staff onboarding across four facilities, patient app launch, leadership reporting dashboards, and telemetry across US and EU deployments.
Beyond the booking-and-records core, the platform carries a reporting subsystem that turns day-to-day clinical activity into an operational picture for leadership. The reports surface appointment volume by day and by clinic, employee performance such as appointments per physician per month, and the status of each staff member across the group, so leadership reasons about the four facilities as one organization rather than four spreadsheets. The same pipeline that records a patient booking or a documented consultation feeds these dashboards, so the numbers leadership sees are the numbers staff generated — no manual roll-up. The subsystem was built with extensibility in mind: adding a new performance metric, a financial-reporting overlay, or a cross-clinic utilization view is a configuration change against the reporting service rather than a code release. It is the layer that turns a clinic management system from a digital appointment book into a planning tool, and it is where the platform earns its keep for healthcare operators who have to commit staffing and capacity decisions weeks in advance across the US and EU.
The system shipped as a single English-language build serving healthcare operators across the United States and the European Union, without a separate codebase per region. It serves clinic groups in California, New York, Texas, Florida, and Washington in the US, and in the Netherlands, Germany, France, Ireland, and Sweden in the EU. Because the client owns its own deployment, data-handling practices are aligned with GDPR for users in the EU and with the US state-privacy patchwork — CCPA / CPRA (California), VCDPA (Virginia), CPA (Colorado), CTDPA (Connecticut), UCPA (Utah), TDPSA (Texas), and Oregon CPA. Role-based access separates administrator, doctor, and leadership views, patient data can be pinned to US or EU infrastructure for future data-residency commitments, and the platform is designed for HIPAA-capable operation where US health-information rules apply — so regional compliance reduces to honest disclosure and access discipline rather than per-jurisdiction rework.
The platform is built to roll out across EU and US clinic groups in parallel, with each facility's web control plane and mobile clients provisioned identically and bound to the local roster of physicians and services. The booking, records, and reporting model runs the same way in every region, so a multi-clinic operator gets one consistent picture across geographies. The engineering team behind the build runs a CET workday with East-Coast US overlap (9 AM–1 PM ET) for stand-ups, rollout choreography, and incident response — the window that lets a US operations team and an EU engineering team share four hours of live overlap every day. Data-handling references are documented directly against GDPR obligations and California CCPA obligations.
The active custom software development roadmap for the clinic platform includes a telemedicine module for remote consultations, deeper financial reporting that turns the appointment ledger into revenue and utilization analytics, and a patient-portal expansion with secure document exchange. A multi-group operations console with cross-clinic referrals is planned for US and EU operators running several facilities, with the role model already structured for additional roles such as nursing and reception. Infrastructure plans include further data-residency automation, a continuous data-integrity harness, and regional deployment scaffolded into the cloud & DevOps roadmap.
If you are planning a medical clinic platform, a patient-booking app, or any healthcare system where patient data has to stay private and role-based across multiple facilities for audiences in the US and EU, we have shipped this stack end-to-end and can compress the build timeline meaningfully. The product overview is available at yusmpgroup.ru (web, iOS, and Android), and the engineering team behind it sits inside YuSMP Group. We work fixed-price for well-scoped MVPs and on dedicated development teams for ongoing delivery, with a CET workday and a guaranteed East-Coast US overlap (9 AM–1 PM ET) window for stand-ups, demos, and incident response.
A clinic-platform MVP covering a patient appointment-booking app, a staff scheduling client, and a web control plane with one role typically costs $110k–$260k. Adding a second mobile platform, role-based admin, doctor, and leadership dashboards, consultation history, verified patient reviews, and analytics brings a full multi-clinic product to $300k–$700k. The dominant cost drivers are the role-based access model, the appointment-conflict logic across clinics and physicians, and the data-protection controls expected for health information in the US and EU.
Off-the-shelf clinic software assumes one practice with a single front desk. A group of independent clinics sharing patients, physicians, and reporting rarely fits that template, and the configuration tax of bending a packaged product to multi-clinic rules often exceeds a custom build. A custom platform lets you model the real organization — separate administrator, doctor, and leadership roles across several facilities — integrate your own scheduling rules, and own the patient data, which matters for US and EU operators with GDPR and CCPA obligations.
Patient and clinical records are the most sensitive data in the system, so access is role-based by default: administrators, doctors, and leadership each see only what their role requires. Because the client owns its own deployment, data can be pinned to US or EU infrastructure for residency, transport and storage are encrypted, and data-handling is aligned with GDPR for EU users and the US state-privacy patchwork for American users. We design for HIPAA-capable operation, but never claim certification that has not been independently completed.
This build separates four perspectives. Patients book appointments, choose physicians, and read verified reviews from real visitors. Administrators manage the appointment and patient database across clinics. Doctors work their personal schedule, open patient cards, and document each visit. Leadership sees analytics, performance metrics, and reporting. Keeping these as distinct role-based views — rather than one shared screen with toggles — is what makes the platform safe to roll out across several independent facilities at once.
A focused MVP with a patient booking app, a staff scheduling client, and a single-role web control plane typically takes 16–24 weeks. Adding the second mobile platform, role-based admin, doctor, and leadership dashboards, consultation history, and reporting analytics adds 10–14 weeks. This project ran roughly 11 months end-to-end because it unified four independent clinics — replacing scattered spreadsheets and paper with one shared platform takes deliberate data-migration and onboarding work.
Related cases
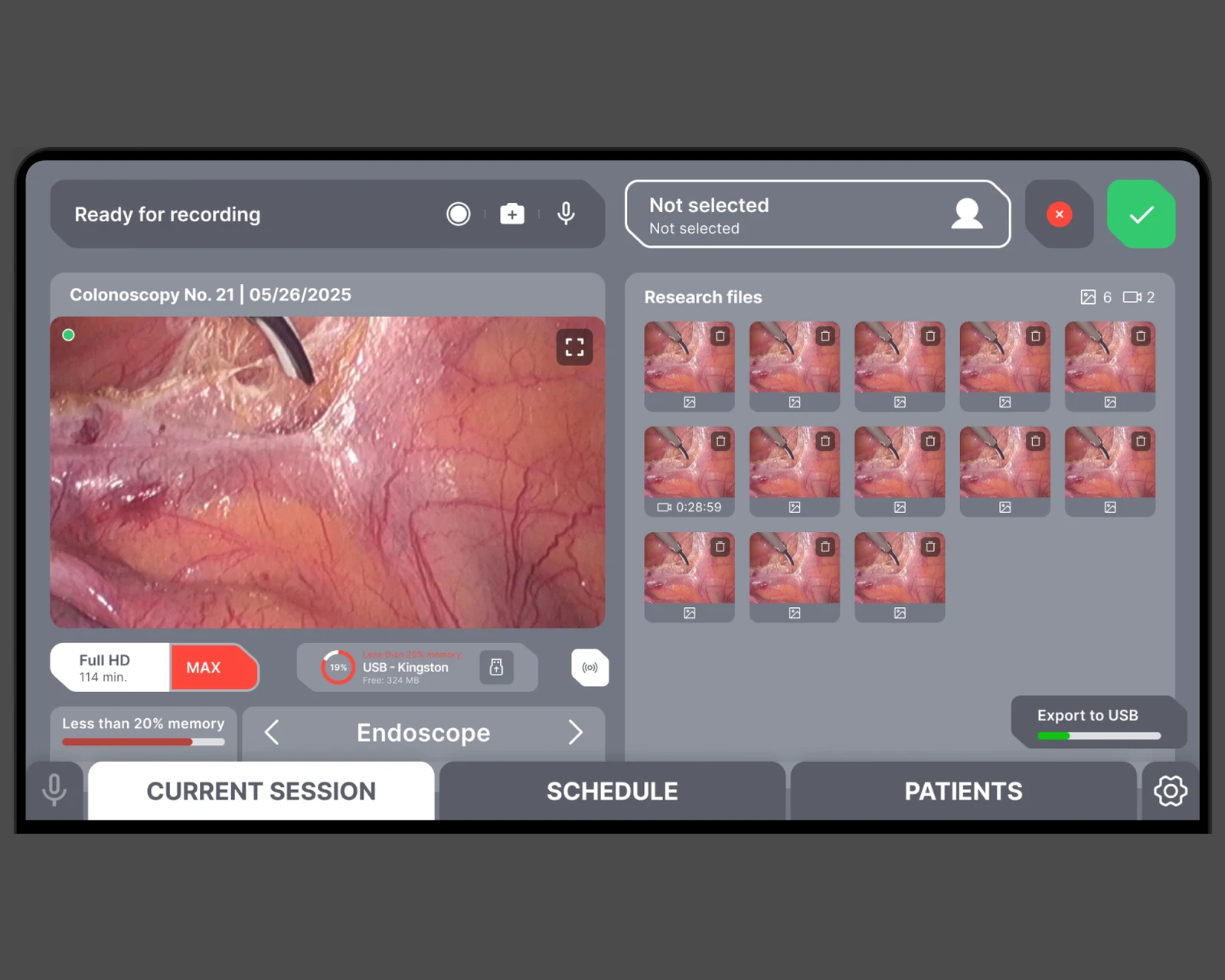
Endoscopy imaging and reporting software for clinical teams, built for diagnostic accuracy across US & EU.
View case →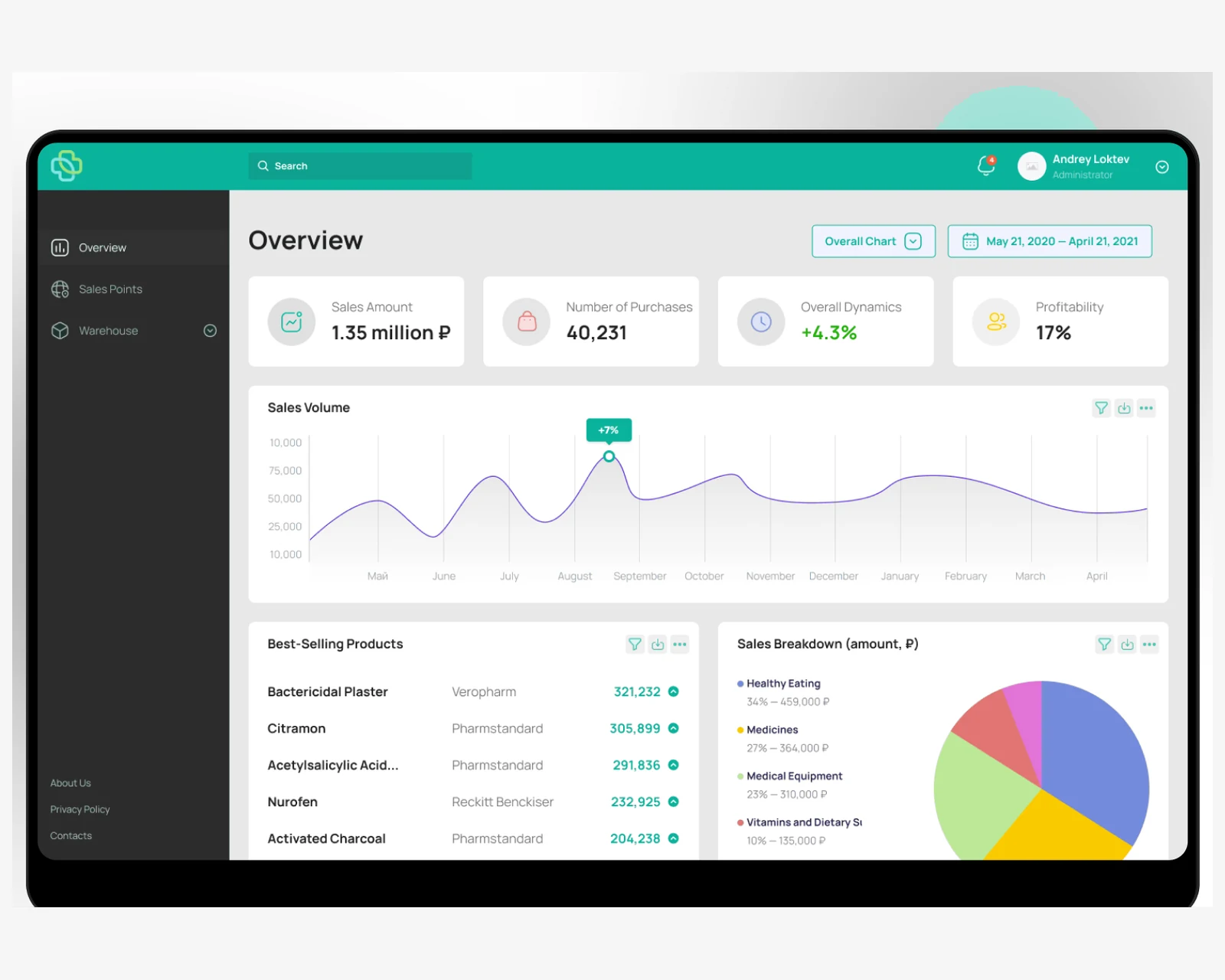
Pharmacy ordering and inventory platform connecting patients and stock management across US & EU.
View case →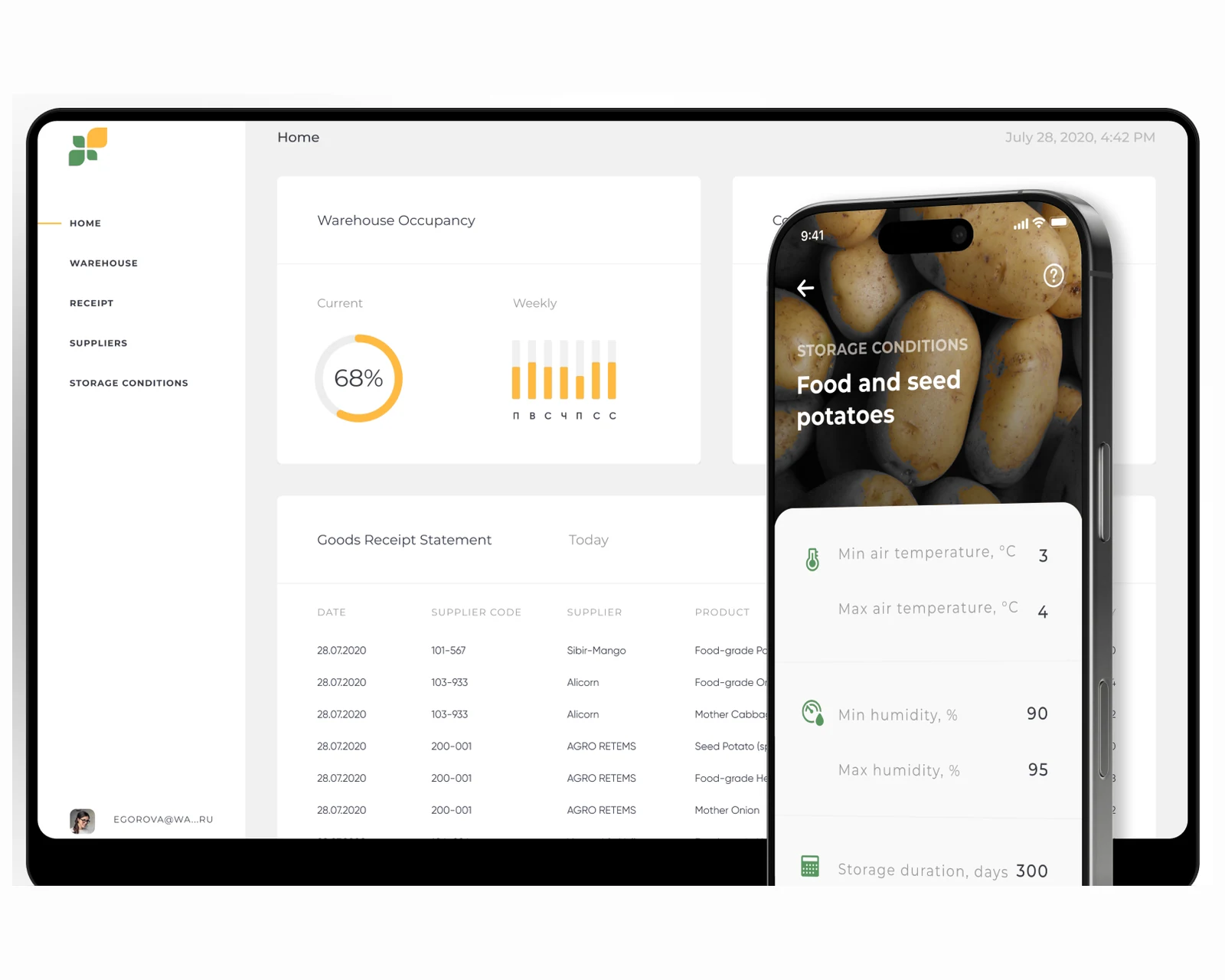
React web control plane and native mobile scanners with role-based access and real-time dashboards across US & EU.
View case →
Custom platforms engineered to your business model, scaling cleanly from MVP to millions of users.
Explore custom software development →
Native iOS, Android, and cross-platform apps with store-ready release pipelines.
Explore mobile app development →
Containerized infrastructure, CI/CD pipelines, and Terraform-managed deployments across US & EU regions.
Explore cloud & DevOps →Share a few details and a senior consultant will reply within one business day.